Overview
That dull misery in the shoulder, knee or elbow known as bursitis can strike anybody, from the couch potato to the highly trained athlete. Though bursitis may hurt as much as arthritis, it isn?t a joint disease. Rather, it's an acute or chronic painful inflammation of a bursa. Bursae (from the Greek word for wine-skin and related to the English word purse) are small, closed, fluid-filled sacs that protect muscles and tendons from irritation produced by contact with bones. If friction becomes too great, from overexercising, hard work, or injury, for instance-the bursae themselves may get inflamed. Though the shoulder is a common locale for bursitis, any of the bursae in the human body-there are approximately 150-can become irritated. Occupational bursitis is not uncommon and is known by old, familiar names such as "housemaid's knee," and "policeman's heel." One of the most common foot ailments, the bunion, is a form of bursitis.
Causes
Bursitis can be caused by an injury, an infection, or a pre-existing condition in which crystals can form in the bursa. Injury. An injury can irritate the tissue inside the bursa and cause inflammation. Doctors say that bursitis caused by an injury usually takes time to develop. The joints, tendons, or muscles that are near the bursae may have been overused. Most commonly, injury is caused by repetitive movements.
Symptoms
A person with bursitis can have one or more of the symptoms below. Pain, the pain increases with movement or pressure. Tenderness is felt even without movement. Swelling. Loss of movement. If the bursitis is caused by an infection it is called Septic Bursitis. The patient with septic bursitis may have the following additional symptoms. Fever. The affected area is red. The affected area feels hot when touched.
Diagnosis
When you suspect you have retrocalcaneal bursitis, your foot doctor will begin by taking a complete history of the condition. A physical exam will also be performed. X-rays are usually taken on the first visit as well to determine the shape of the heel bone, joint alignment in the rearfoot, and to look for calcium deposits in the Achilles tendon. The history, exam and x-rays may sufficient for your foot surgeon to get an idea of the treatment that will be required. In some cases, it may be necessary to get an ultrasound or MRI to further evaluate the Achilles tendon or its associated bursa. While calcium deposits can show up on xray, the inflammation in the tendon and bursa will show up much better on ultrasound and MRI. The results of these tests can usually be explained on the first visit. You can then have a full understanding of how the problem started, what you can do to treat prevent it from getting worse/ You will also know which treatment will be most helpful in making your heel pain go away.
Non Surgical Treatment
Orthotics may assist heel bursitis by providing stability to the heel, reduce any foot functioning abnormalities and provide extra support for the feet. The orthotic achieves this by maintaining correct foot posture, therefore facilitating normal functioning of the Achilles tendon. Icing the back of the heel post activity for temporary relief. Non-steroidal anti-inflammatory medication such as ibuprofen can reduce inflammation of the bursa. Stretching of the calf muscle may reduce the pulling on the heel by the Achilles tendon. Shoes that have an elevated heel may reduce pulling on the heel from the Achilles tendon. Resting the painful heel may reduce inflammation and pain. Surgical removal of the painful bursa is a last resort treatment when all other treatments have failed.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Prevention
Protect that part of the body that may be most vulnerable, If you have to kneel a lot, get some knee pads. Elbow braces can protect tennis and golf players. If you are an athlete or avid walker, invest in some good walking or running shoes. When doing repetitive tasks have breaks. Apart from taking regular breaks, try varying your movements so that you are using different parts of your body. Warm up before exercise. Before any type of vigorous exercise you should warm up for at least 5 to 10 minutes. The warm up could include walking at a good speed, slow jogging, or a cycling machine. Strong muscles add extra protection to the area. If you strengthen the muscles in the area where you had bursitis (after you are better), especially the area around the joint, you will have extra protection from injury. Make sure you do this well after your bursitis has gone completely.
That dull misery in the shoulder, knee or elbow known as bursitis can strike anybody, from the couch potato to the highly trained athlete. Though bursitis may hurt as much as arthritis, it isn?t a joint disease. Rather, it's an acute or chronic painful inflammation of a bursa. Bursae (from the Greek word for wine-skin and related to the English word purse) are small, closed, fluid-filled sacs that protect muscles and tendons from irritation produced by contact with bones. If friction becomes too great, from overexercising, hard work, or injury, for instance-the bursae themselves may get inflamed. Though the shoulder is a common locale for bursitis, any of the bursae in the human body-there are approximately 150-can become irritated. Occupational bursitis is not uncommon and is known by old, familiar names such as "housemaid's knee," and "policeman's heel." One of the most common foot ailments, the bunion, is a form of bursitis.
Causes
Bursitis can be caused by an injury, an infection, or a pre-existing condition in which crystals can form in the bursa. Injury. An injury can irritate the tissue inside the bursa and cause inflammation. Doctors say that bursitis caused by an injury usually takes time to develop. The joints, tendons, or muscles that are near the bursae may have been overused. Most commonly, injury is caused by repetitive movements.
Symptoms
A person with bursitis can have one or more of the symptoms below. Pain, the pain increases with movement or pressure. Tenderness is felt even without movement. Swelling. Loss of movement. If the bursitis is caused by an infection it is called Septic Bursitis. The patient with septic bursitis may have the following additional symptoms. Fever. The affected area is red. The affected area feels hot when touched.
Diagnosis
When you suspect you have retrocalcaneal bursitis, your foot doctor will begin by taking a complete history of the condition. A physical exam will also be performed. X-rays are usually taken on the first visit as well to determine the shape of the heel bone, joint alignment in the rearfoot, and to look for calcium deposits in the Achilles tendon. The history, exam and x-rays may sufficient for your foot surgeon to get an idea of the treatment that will be required. In some cases, it may be necessary to get an ultrasound or MRI to further evaluate the Achilles tendon or its associated bursa. While calcium deposits can show up on xray, the inflammation in the tendon and bursa will show up much better on ultrasound and MRI. The results of these tests can usually be explained on the first visit. You can then have a full understanding of how the problem started, what you can do to treat prevent it from getting worse/ You will also know which treatment will be most helpful in making your heel pain go away.
Non Surgical Treatment
Orthotics may assist heel bursitis by providing stability to the heel, reduce any foot functioning abnormalities and provide extra support for the feet. The orthotic achieves this by maintaining correct foot posture, therefore facilitating normal functioning of the Achilles tendon. Icing the back of the heel post activity for temporary relief. Non-steroidal anti-inflammatory medication such as ibuprofen can reduce inflammation of the bursa. Stretching of the calf muscle may reduce the pulling on the heel by the Achilles tendon. Shoes that have an elevated heel may reduce pulling on the heel from the Achilles tendon. Resting the painful heel may reduce inflammation and pain. Surgical removal of the painful bursa is a last resort treatment when all other treatments have failed.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Prevention
Protect that part of the body that may be most vulnerable, If you have to kneel a lot, get some knee pads. Elbow braces can protect tennis and golf players. If you are an athlete or avid walker, invest in some good walking or running shoes. When doing repetitive tasks have breaks. Apart from taking regular breaks, try varying your movements so that you are using different parts of your body. Warm up before exercise. Before any type of vigorous exercise you should warm up for at least 5 to 10 minutes. The warm up could include walking at a good speed, slow jogging, or a cycling machine. Strong muscles add extra protection to the area. If you strengthen the muscles in the area where you had bursitis (after you are better), especially the area around the joint, you will have extra protection from injury. Make sure you do this well after your bursitis has gone completely.
 Overview
Overview Symptoms
Symptoms Prevention
Prevention Overview
Overview Symptoms
Symptoms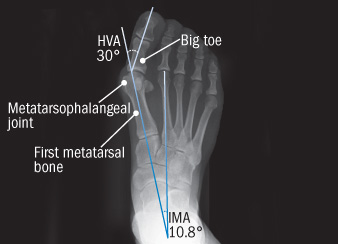 Knowing how bunions develop is helpful in selecting the appropriate bunion treatment. In general, most bunion deformities are a result of foot structure and function which are genetic. As the heel strikes the ground when walking, the joints of the foot unlock and absorb impact. Referred to as pronation, the arch collapses causing the feet to flatten. This flattening causes excessive tension of the tendon in the upper mid-foot that enables the big toe to bend upward. The tendon contracts which then forces the big toe to be pulled laterally toward the second toe. It can take many years for a bunion to develop, and especially to the point of pain. One can have a bunion but not yet experience any bunion pain. Conversely, one can suffer from bunion pain without having a severe deformity.
Knowing how bunions develop is helpful in selecting the appropriate bunion treatment. In general, most bunion deformities are a result of foot structure and function which are genetic. As the heel strikes the ground when walking, the joints of the foot unlock and absorb impact. Referred to as pronation, the arch collapses causing the feet to flatten. This flattening causes excessive tension of the tendon in the upper mid-foot that enables the big toe to bend upward. The tendon contracts which then forces the big toe to be pulled laterally toward the second toe. It can take many years for a bunion to develop, and especially to the point of pain. One can have a bunion but not yet experience any bunion pain. Conversely, one can suffer from bunion pain without having a severe deformity.


 Achilles tendon rupture is most common in people aged 30-50. Patients may describe the injury as feeling or hearing a snap or bang, or as feeling they have been shot in the back of the leg. On examination, patients will have reduced plantarflexion and a positive Thompson test. Surgery is associated with a lower risk of re-rupture and a greater likelihood of returning to sporting activity. Conservative management reduces the chance of complications.
Achilles tendon rupture is most common in people aged 30-50. Patients may describe the injury as feeling or hearing a snap or bang, or as feeling they have been shot in the back of the leg. On examination, patients will have reduced plantarflexion and a positive Thompson test. Surgery is associated with a lower risk of re-rupture and a greater likelihood of returning to sporting activity. Conservative management reduces the chance of complications.



.jpg)


